

With eminent scientists continuing to challenge the truth of everything we were told about the ‘pandemic,’ Rebekah Barnett looks at the latest ‘vaccine’ development, ‘immune printing.’
__________________________________________________________
New booster, old immune response: as Australia surfs its eighth COVID wave, scientists say boosters could be making COVID infections worse.
For several years now, experts in vaccinology and immunology have been warning of the risks of immune imprinting, otherwise known as original antigenic sin, with repeat dosing of the COVID vaccines.
Immune imprinting occurs “when repeat exposure to antigens reduces the ‘power’ of the immune response,” explains Dr Jessica Rose, a Canadian researcher with a Masters in Immunology and a Post-Doctoral degrees in Molecular Biology and Biochemistry.
“It’s a ‘first impressions matter’, kind of thing,” she says. “The immune response – once effective against a specific set of antigens in a pathogen – may become ‘stuck in the ‘80s’ to antigenically-similar pathogens that come from the ‘90s. Thus, the individual will not be producing the most effective antibodies against the ‘new’ antigens.”
What this means out in the real world is that, when encountering a new variant (e.g.: the grandchild of Omicron), a person vaccinated against an older variant (e.g.: the Wuhan strain) will mount an immune response targeted to the older variant. It’s the ‘90s, but your immune response is stuck in the ‘80s.

Initially, COVID vaccines targeted to the original Wuhan strain were intended to “prevent coronavirus disease,” as stated in the Therapeutic Goods Administration’s (TGA) Public Assessment Report for the mRNA Pfizer vaccine, for example.
With the arrival of Omicron and the fast-waning efficacy of the primary series COVID vaccines, however, the public health response pivoted to ‘variant chasing’ with bivalent boosters, and the revised aim of reducing severity of symptoms and likelihood of death.
The pivot to regular boosting prompted apprehension within the scientific community over the potential for immune imprinting to reduce vaccinated people’s capacity to fight off new variants.
As early as January 2022, it was reported that the Head of Vaccines Strategy at the European Medicines Agency (EMA), Marco Cavaleri, had “raised concerns that a strategy of giving boosters every four months hypothetically poses the risk of overloading people’s immune systems and leading to fatigue in the population.”
In April 2022, US-based paediatrician and vaccine expert and advocate Dr Paul Offit warned in an editorial published in the New England Journal of Medicine (NEJM), that Covid boosters are “not risk-free,” and that original antigenic sin “could limit our ability to respond to a new variant.”
Then in February 2023, Dr Offit penned another editorial for the NEJM, this time questioning the benefit of bivalent boosters for anyone other than the elderly, or patients with multiple comorbidities, after bivalent booster trials were found to have produced “underwhelming” results.
Dr Offit wrote, “Why did the strategy for significantly increasing BA.4 and BA.5 neutralizing antibodies using a bivalent vaccine fail? The most likely explanation is imprinting. The immune systems of people immunized with the bivalent vaccine, all of whom had previously been vaccinated, were primed to respond to the ancestral strain of SARS-CoV-2.”
The test subjects’ immune responses were stuck in the 80s.
“I believe we should stop trying to prevent all symptomatic infections in healthy, young people by boosting them with vaccines containing mRNA from strains that might disappear a few months later,” concluded Dr Offit.
Dr Rose agrees that waning efficacy of the COVID vaccines “is likely due to this concept of immune imprinting,” combined with the additional risk of immune tolerance due to an antibody ‘class switch.’
Dr Rose refers to research showing that as patients receive additional doses of COVID mRNA vaccines, their immune response can ‘switch’ from producing more of the antibodies that fight off viral infections (good!), to instead producing more of an antibody type called IgG4, which instructs the immune system to tolerate the antigen (not so good).
“This means that instead of fighting the actual pathogen upon stimulation, the immune system will say: meh,” says Dr. Rose. People suffering immune tolerance due to the IgG4 class switch may therefore have greater difficulty clearing the virus after they become infected.
A preprint study published in January of this year provides an indication that the antibody class switch may be more of a concern with the mRNA vaccines in particular compared to other COVID vaccines using traditional technology.
It was therefore conspicuous when a senior doctor and advisor on Australia’s National Clinical Evidence Taskforce for treatment of COVID, Professor Mark Morgan, admitted to a Senate Committee earlier this month that he had “never heard of” immune imprinting.
During a hearing for an inquiry into the appropriate Terms of Reference for a prospective COVID Royal Commission, on 1 February, Senator Nita Green noted that COVID was still a concern for vulnerable Australians, and asked Prof Morgan to comment on how to address this risk.
“There’s an ongoing need to make available and inform people about the availability of vaccine boosters, of antiviral treatment… and an ongoing need to remind people of the lessons we learned about personal protection and avoiding the spread of infections,” said Prof Morgan, who was present in his capacity as a Fellow of the Royal Australian College of General Practitioners (RACGP), where he is Chair of the Expert Committee for Quality Care.
The RACGP is the peak body for General Practitioners (GPs, similar to PCPs or family doctors in the US) in Australia, overseeing training and, and was a primary source of information for GPs during the pandemic and vaccine rollout.
Senator Gerard Rennick followed, commenting that “the medical profession has continued to promote boosters, knowing that viruses mutate. What’s your comment in regards to the failure to alert people to the risks of immune imprinting?”
“I’ve never heard of the word immune imprinting until you mentioned it,” responded Prof Morgan candidly.
Dr Rose is unsurprised. “To be perfectly frank, unless GPs actively seek out immunological training, they will not have it,” she says. “There is also almost no training for GPs in vaccinology, which begs the question: Why are GPs giving so many vaccines without knowing basic concepts in immunology or vaccinology?”
Tasmanian Medical Doctor and Co-Director of multidisciplinary group Australians for Science and Freedom (ASF), Dr Julie Sladden is of a similar view. It’s an important concept in viral immunology and vaccinology, but not really something you see discussed routinely in general practice medical education,” she says.
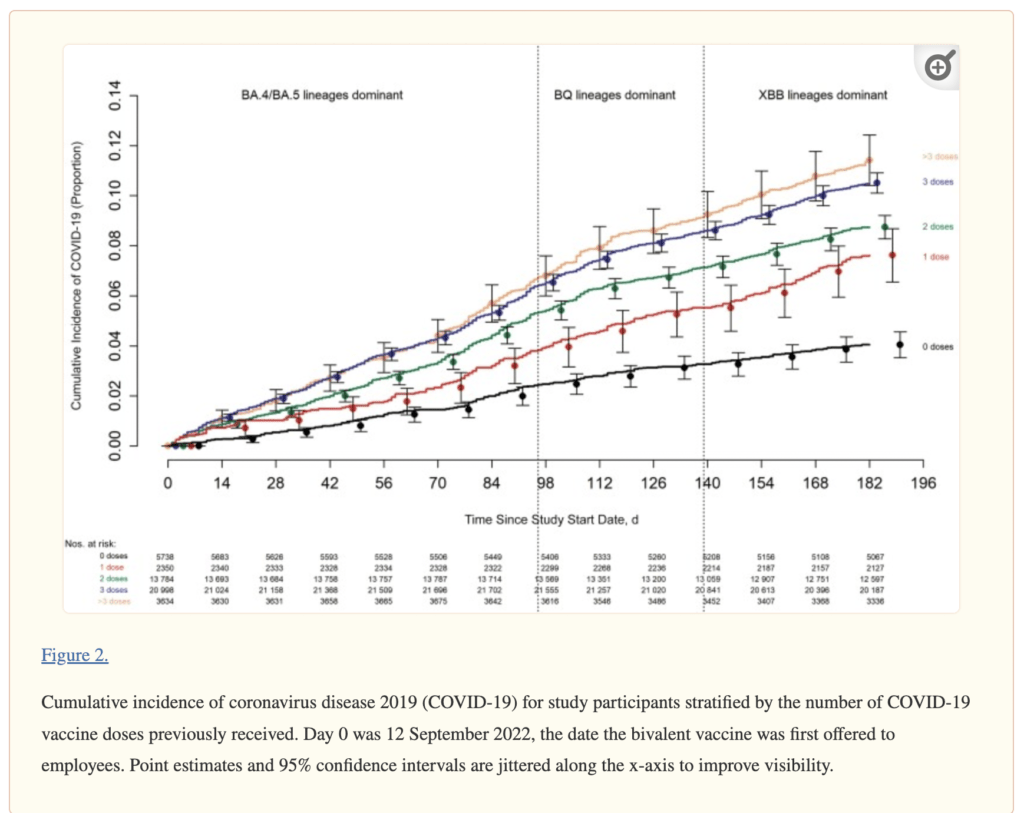
“As a doctor, I did not see anything come across my desk about immune imprinting, or information like the Cleveland Clinic study which showed that people with more COVID-19 vaccinations were more likely to get infected.”
Dr Sladden says that GPs being uninformed about the Covid vaccines cuts to the heart of informed consent, a point she made as a witness in the Senate Committee hearing as a representative of both ASF, and the People’s Terms of Reference, a declaration signed by more than 48,000 Australians.
“There has been a lot of trust from the doctors being placed in the regulation bodies and authorities to the point where I would say that a lot of doctors don’t understand the way the vaccines work, and the potential for adverse effects with repeated doses,” says Dr Sladden.
Dr Sladden notes that the mRNA technology used in the Moderna and Pfizer vaccines is different from traditional vaccines, and carries unique risks, particularly concerning repeat dosing, the effects of which have been relatively undertested.
“We never boosted traditional vaccines every six months. This is new, and because doctors don’t fully understand the risks, there has been a mass lack of informed consent for patients,” she says.
Addressing the Senate Committee earlier this month, Dr Sladden told Senators that the Covid response had revealed “a catastrophic failure of medical ethics and human rights,” and “wholesale removal of informed consent.”
“Millions of Australians were vaccinated with a product they couldn’t properly consent to, by doctors who didn’t fully know the risks. We need a Royal Commission to find out what went wrong, and make sure it never happens again,” she told those present.
Dr Astrid Lefringhausen, a Molecular Biologist and Biochemist with training in immunology and virology, echoes Dr Sladden’s calls for a Royal Commission, and would like to see Australia’s COVID booster advice take the full scope of risks into account.
Dr Lefringhausen and Dr Rose are both signatories on the Peoples Terms of Reference for a Royal Commission into Australia’s COVID response, and both scientists conducted research referenced in the document.
Dr Lefringhausen has co-authored a number peer-reviewed of papers on COVID and its treatments, including a systematic review of the COVID vaccines published in the Journal of Clinical and Experimental Immunology, and a paper exploring the pathogenicity of the COVID-19 spike protein in from both the virus and vaccine mRNA, a phenomenon that the authors call ‘spikeopathy,’ in the journal Biomedicines. The spikeopathy paper is the most viewed publication in the journal’s history.
“The problem is, people don’t seem to understand that with boosters, your body makes the same spike protein as the virus.” Additional doses have the effect of “flooding your body” with spike protein, says Dr Lefringhausen, pointing to research showing the presence of vaccine-produced spike protein in patient’s bodies 60 days after vaccination (the study was ended at 60 days).
Because the spike protein is toxic, people should “think of a booster like an infection, a very bad infection, and try to minimise exposure” to both boosters and infections, says Dr Lefringhausen.
However, whereas repeat exposure to boosters “[push] you towards immune tolerance and more infections,” Dr Lefringhausen points out that natural infection leads to a “more rounded” immune response, better preparing the infected person to mount a strong immune response at the next exposure.
Due to chopping and changing in surveillance efforts and record keeping, it is hard to say how many Australians have natural immunity to COVID, and which age groups have received how many boosters.
But we do know that by the end of 2022, more than two-thirds of Australian adults had been infected with COVID at least once (mostly Omicron), according to serosurveillance data. During the same period, adult primary series vaccine coverage climbed to well over 90 per cent, and booster coverage reached approximately 70 per cent and 40 per cent for the third and fourth doses, respectively.
This serosurveillance work was subsequently discontinued, and there does not appear to be an alternative co-ordinated effort to track infection and reinfection rates in Australia, so the number and severity of reinfections is unknown.
However, a recent spate of media reports sharing anecdotal accounts of people experiencing multiple infections, severe infections, or ongoing (long) symptoms is suggestive that for some Australians, their immune response is stuck in the 80s.
“More vaccine doses is leading to immune system impairment. Telling people to keep vaccinating is basically telling them to commit suicide,” says Dr Lefringhausen, who believes that the public health response to COVID has been “nothing but disastrous for a lot of Australians.
Dr Lefringhausen is of the view that this is exactly why we need a Royal Commission into Australia’s COVID response. “You can’t just let this go… because if we don’t work out what happened and how, it will happen again.”

